
本記事は英文ブログを日本語に翻訳再編集(一部追記を含む)したものです。本記事の正式言語は英語であり、その内容・解釈については英語が優先します。
CHRIS LEWIS
Primary research manager, U.S. Access & Reimbursement, Clarivate
COVID-19パンデミックに伴う遠隔医療サービスへの需要の高まりを受けて、デジタルセラピューティクス(DTx)ソリューションが市場に急増しており、米国のペイヤーや薬局給付管理者は、薬局給付や医療給付に必ずしも適合しないこれらの製品をカバーするか否か、またどのようにカバーすべきかについて頭を悩ませています。クラリベイトのAccess & Reimbursement担当エキスパートであるクリス・ルイスが、2021年に開催されたAMCP(Academy of Managed Care Pharmacy)の年次会議で議論された主な内容を紹介します。
DTxとは、特定の病気や障害を予防、管理、治療するためのソフトウェアプログラムによるエビデンスに基づいた治療的介入のことです。よく知られている例としては、WellDoc社の糖尿病管理用BlueStarや、Pear Therapeutics社の物質・オピオイド依存症用認知行動療法(reSETおよびreSET-O)、不眠症用認知行動療法(Somryst)などがあります。
ペイヤーやプロバイダーは、市場に出回っている30万ものデジタルヘルス・ソリューション1を吟味し、これらの製品を保険プランでカバーするための独自のアプローチを生み出しています。この点に関してCigna社の医療サービス部門であるCare Solutions Evernorthのバイスプレジデント兼ゼネラルマネージャーであるSnezana Mahon氏(PharmD)は次のように述べています。Mahon氏と、ミネソタ州に本拠地を置く商業医療プランPreferredOneの薬局担当副社長Samir Mistry氏(PharmD)は、AMCPの会議で、デジタルセラピューティクスへの保険適用に対するアプローチを説明しました。
薬局の未来は、身を乗り出して前に進み、これは新しいこと、これは違うこと、ガイドブックもなければ青写真もない、誰もやったことがないことを理解することです
Snezana Mahon, PharmD, Care Solutions Evernorth社 副社長兼ゼネラルマネージャー
不眠症治療薬に関するクラリベイトのAccess & Reimbursementによると、調査対象となった薬局および医療機関のディレクターの10人に9人が、自分たちのマネージドケア組織(MCO)がDTxをカバーするためのポリシーをすでに導入しているか、2021年6月までに導入する予定であると回答しています。
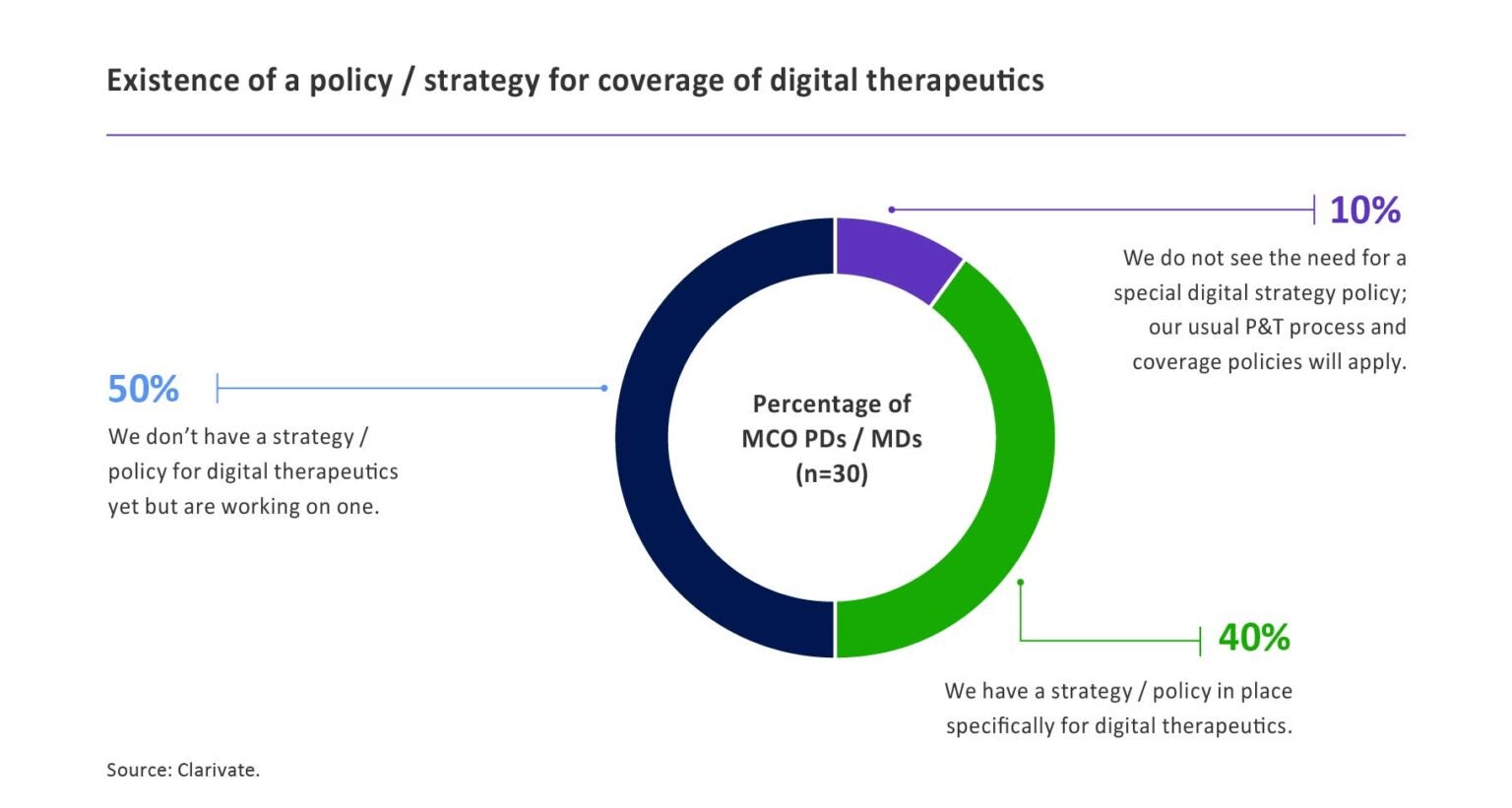
出典: Clarivate Access & Reimbursement、2020年6月
ペイヤーはDTxの臨床的・経済的側面を評価
WellDoc社やPear Therapeutics社の製品など、一部の製品はFDAの承認を得て処方されていますが、多くの製品はこの経路をとっておらず、厳密な無作為化比較臨床試験で検討されていません。「臨床試験データがないものについては、ペイヤーは査読付きの研究、ホワイトペーパー、その他の利用可能な研究を利用することになるだろう」とMahon氏は述べています。PreferredOneとEvernorthの両社は、製品を評価し、市場の受容性を測るために、臨床医、薬剤師、コンサルタント、ブローカー、ITチーム、エンドユーザーなど、複数の関係者に相談しています。
経済的評価では、製品のコストとメリットを比較し、次のように問いかけます:
- その製品は治療の中でどのような役割を果たしているのか、アンメットニーズを満たしているのか、ケアのギャップを解消しているのか。
- その製品はアドヒアランスを向上させ、病院での使用やポリファーマシーを減らすことができるか?
- その製品は、患者の治療にかかる総コストを削減できるか?
重要な検討事項の一つは、医師とその患者が実際にDTxを使用するかどうかです:
- デバイスやプラットフォームは、簡単に理解でき、使いやすく、患者の健康指標を効果的に医師に届けることができるか?
- また、そのデータを医師のEMRワークフローに統合できるか?
- エンドユーザーをターゲットにした市場参入戦略やコミュニケーション戦略を持っているか?
薬局経由と医療給付経由の補償を評価する
業界全体での指針がないため、多くのプランではDTxを給付に割り当てるために独自の工夫がなされています。Express Scripts社のPBMを利用しているプランスポンサーは、薬局での保険適用のためにカスタマイズ可能なデジタルフォーミュラリーを利用することができます。Mahon氏は、新しいデジタル保険給付を作りたいという顧客もいると指摘します。しかし、ほとんどのDTxは、薬局給付または医療給付(またはその両方)でカバーされるという点では一致しているようです。
「この決定は製品の調達方法に影響されることが多い」とMistryは述べています。PreferredOneでは、DMEに分類される製品やメーカーから直接仕入れた製品、オフィス訪問時に使用する製品、専門家やケースマネージャーの介入が必要な製品については、医療給付を使用する傾向にあります。また、PBMが薬局側との契約を制限しているプランでは、DTxを医療保険でカバーすることもあります。
薬局での保険適用は、処方箋ベースのDTxに適している傾向がある。また、薬局を経由することで、会員の費用負担が容易になり、薬局を含めた会員との複数のタッチポイントを提供することができます。
契約とデータ収集が鍵となる
プランによっては、リベート契約やリスクベース契約など、製薬メーカーと同様にDTx提供企業と契約を結ぶことになるでしょう。Mistry氏によると、PreferredOne社は、いくつかのベンダーとの間で、特定のパフォーマンス・ベンチマークを満たすことを条件とした価値ベースの契約に取り組んでいます。例えば、治療の中止率が高かったり、ケアの総コストを削減できなかったりすると、プランへの返金が発生する可能性があります。
バリューベース契約では、医療費や薬剤費の請求データ、患者が報告した結果など、多くのデータ要素を統合する必要があります。実際、DTxを成功させるためには、HIPPAに関連する患者のプライバシー問題を解決し、データのセキュリティを確保するだけでなく、医療エコシステム全体でデータを収集し、共有することが不可欠です。これらのデータを取り込むことは、業界が克服しようとしている最大の課題の一つです。
このブログ記事のインサイトは、2021年4月に開催されたAMCP(Academy of Managed Care Pharmacy)会議でのプレゼンテーションや議論をクラリベイトが分析したものと、クラリベイトのAccess & Reimbursementの医師やペイヤーの調査に基づいています。
支払者の政策が医師の処方行動に与える影響に関するブランドレベルの知見が、市場参入戦略を最適化をサポートします。
参考文献:1.Research2Guidance, HealthXL



