| Utilization (2015 – 2019 CAGR) | Clinical value / limitations | Appropriate use criteria (AUCs) | Payer management (PAs and restrictions) | Provider (cardiology vs radiology) control | Site of service (facility) profitability | |||
|---|---|---|---|---|---|---|---|---|
| Stress Echo | arrow_back | Moderate utilization, negative growth | Moderate clinical value, low limitations | AUC consultation not required | Most accessible cardiac imaging tests based on insurance coverage | Always controlled by cardiology | MPI-SPECT/PET reimbursement rates are more than double the stress echo | arrow_forward |
| MPI-PET | Low utilization, moderate growth | High clinical value, moderate limitations | AUC reserves to certain patient populations or as second line test | PA process is highly restrictive towards PET | PET scanners are less common in OICs & typically owned by oncology in hospitals | MPI-PET can be very profitable in high volume practices | ||
| MPI-SPECT | High utilization, negative growth | High clinical value, low limitations | AUC prefers SPECT relative to PET for nuclear imaging | Most payers require a PA for MPI-SPECT | Many cardiology departments/OICs have their own dedicated SPECT machines | Reimbursement is significantly higher than stress-echo and comparable to PET in the hospital setting | ||
| CCTA Only | Low utilization, high growth | Moderate clinical value, low limitations | AUC generally relegates to second line test | Increasing coverage of CCTA as a ‘first line’ test for CAD evaluation | PET scanners are less common in OICs & typically owned by other departments in hospitals | Significantly lower reimbursement, but similar costs, to nuclear imaging – low profitability | ||
| CCTA + FFRCT | Low utilization, high growth | High clinical value, moderate limitations | AUC generally relegates to second line test | Coverage criteria requires an inconclusive or non-diagnostic CCTA result | Controlled by FFRct manufacturer (HeartFlow) | Reimbursement for FFRct is paid directly to HeartFlow |
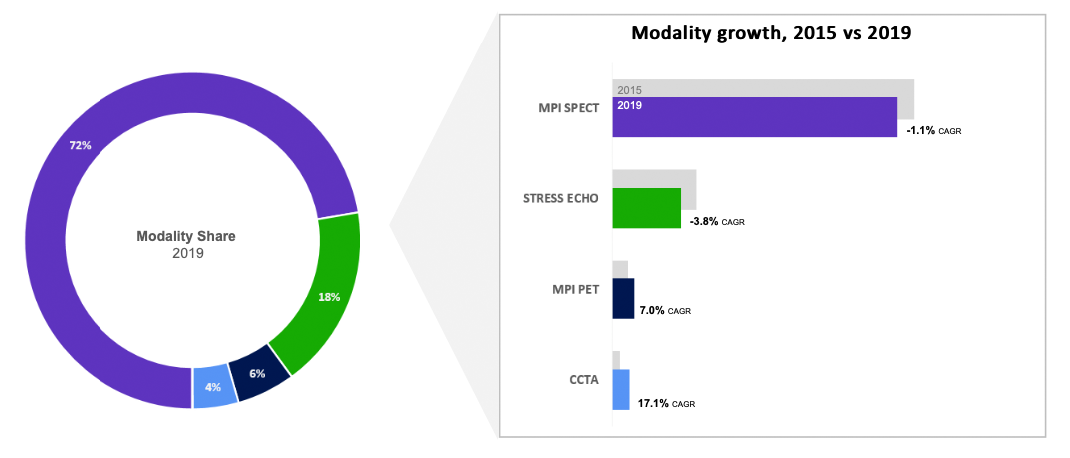
Utilization (2015 – 2019 CAGR)